

Background
The median age of diagnosis of chronic lymphocytic leukemia (CLL) in the US is 70 years, and less than 2% of patients (pts) are diagnosed before age 45. No prior studies have investigated adolescent and young adult (AYA) pts with CLL in the era of next generation sequencing (NGS) gene mutation analysis and novel oral therapies. This retrospective study examines disease characteristics that affect outcomes of AYA pts with CLL, including those treated with novel agents.
Methods
Pts aged 15 to 39 years at the time of diagnosis of CLL/SLL, diagnosed between 1/1/2000 and 12/31/2019, and evaluated at least once at our institution (MDACC) were included in the analysis. The primary objective was to evaluate how disease characteristics predict outcomes for AYA pts with CLL. Baseline characteristics (labs, Rai stage) were recorded if documented pre-treatment and within 12 months of diagnosis; other characteristics (FISH, cytogenetics, CD38, ZAP-70, gene mutations) could be documented any time pre-treatment. IGHV mutation status could be documented at any time. The outcomes of pts who received novel oral agents (defined as BTK, BCL2, or PI3K inhibitors) at any time during their disease course were specifically evaluated as a secondary objective. Time-to-first treatment (TTFT) was assessed as the time from CLL diagnosis to start of first therapy. Overall survival (OS) was assessed as the time from CLL diagnosis to death from any cause.
Results
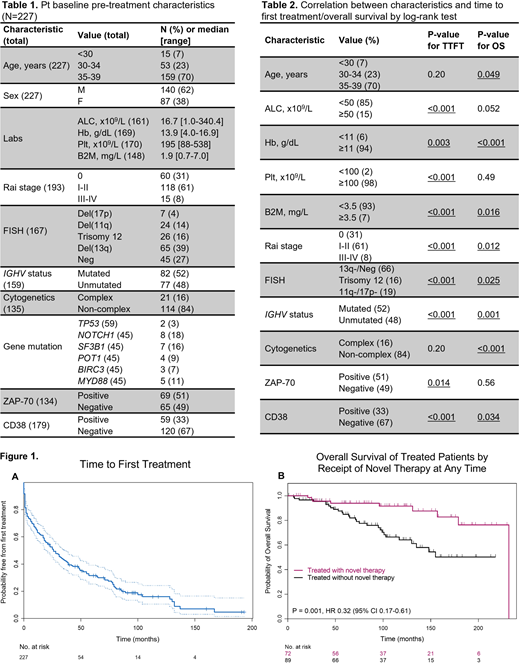
A total of 227 pts were identified and summarized. Median age at diagnosis was 37 years (range, 17-39). Median follow-up time from diagnosis was 7.1 years (range, 0-19.3) with data cutoff as of 6/30/2020. Baseline characteristics are described in Table 1. Pre-treatment hierarchical FISH categories were as follows for 167 pts with available data: 65 (39%) had del(13q), 26 (16%) trisomy 12, 24 (14%) del(11q), 7 (4%) del(17p), and 45 (27%) no FISH abnormality. Of the 159 pts with available data, 82 (52%) had mutated and 77 (48%) unmutated IGHV. A first degree relative with CLL was present for 3% of pts. Gene mutation was identified in 2/59 (3%) of pts for TP53, 8/45 (18%) NOTCH1, 7/45 (16%) SF3B1, 4/45 (9%) POT1, 3/45 (7%) BIRC3, and 5/45 (11%) MYD88 (due to limited number of pts with available gene mutation data, outcomes by mutation status were not analyzed).
A total of 161 (71%) pts received CLL treatment, and median TTFT was 26 months (Fig. 1A). A total of 39 (17%) pts died, and 5- and 10-year OS rates were 90% and 78%, respectively. Characteristics predictive of TTFT and OS are described in Table 2. A total of 72 (32%) pts received novel therapy at any time during their disease course, and 89 (39%) pts were treated only with agents other than novel therapies during their entire treatment course. As expected, OS was longer for pts who received novel therapy at any time vs. pts who did not (p=0.001, hazard ratio 0.32, Fig. 1B), with a 10-year OS rate of 92% vs. 64%, respectively. Pts who received novel therapies were diagnosed later (the median year of diagnosis was 2010 for pts treated with novel therapies, and 2003 for pts treated without novel therapy). All other baseline characteristics were similar between the two groups. The survival advantage of novel therapy exposure was lost when only evaluating treated pts with mutated IGHV (p=0.63).
A total of 18 (8%) pts underwent allogeneic stem cell transplant (allo-SCT). Pts aged <30 (p=0.03) and with del(11q) or del(17p) (p=0.007) were more likely to undergo allo-SCT. A total of 10 (4%) pts developed Richter's transformation (RT). Pts aged <30 (p=0.02) and with del(11q) or del(17p) (p=0.03) had higher risk of RT. t-MDS/AML developed in 3 (1%) pts; all had received prior chemoimmunotherapy. A second primary malignancy, excluding non-melanoma skin cancer, occurred in 8 (4%) pts.
Discussion
This retrospective analysis is the first to evaluate AYA pts with CLL in the era of NGS gene mutation analysis and widespread utilization of novel oral agents. Most prognostic laboratory and molecular markers established in older adults pts with CLL were predictive for young pts as well. Notably, OS was improved for treated pts who received novel therapies at any time during their disease course. The benefit of novel therapy seemed to be lost when analyzing IGHV mutated pts only. This study suggests that novel therapies should be considered as the preferred treatment choice over chemotherapy for AYA pts with CLL, especially for pts with unmutated IGHV.
Sasaki:Otsuka: Honoraria; Novartis: Consultancy, Research Funding; Daiichi Sankyo: Consultancy; Pfizer Japan: Consultancy. Thompson:Janssen-Cilag: Honoraria; Adaptive Biotechnologies: Consultancy, Research Funding; Genentech: Consultancy; Pharmacyclics: Research Funding; AbbVie: Research Funding. Burger:TG Therapeutics: Research Funding, Speakers Bureau; Janssen Pharmaceuticals: Consultancy, Speakers Bureau; AstraZeneca: Consultancy; Gilead Sciences: Consultancy, Research Funding; Beigene: Research Funding, Speakers Bureau; Pharmacyclics, an AbbVie company: Consultancy, Research Funding, Speakers Bureau. O'Brien:Gilead, Pharmacyclics, TG Therapeutics, Pfizer, Sunesis: Consultancy, Research Funding; Kite, Regeneron, Acerta: Research Funding; Amgen, Astellas, Celgene, GlaxoSmithKline, Janssen Oncology, Aptose Biosciences Inc. Vaniam Group, AbbVie, Alexion, Verastem, Eisai, Juno Therapeutics, Vida Ventures: Consultancy. Jain:Pharmacyclics: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; AbbVie: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Genentech: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; AstraZeneca: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; BMS: Research Funding; Pfizer: Research Funding; ADC Therapeutics: Research Funding; Incyte: Research Funding; Servier: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Cellectis: Research Funding; Verastem: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Adaptive Biotechnologies: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Precision Bioscienes: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Fate Therapeutics: Research Funding; Aprea Therapeutics: Research Funding; Janssen: Honoraria, Membership on an entity's Board of Directors or advisory committees; TG Therapeutics: Honoraria, Membership on an entity's Board of Directors or advisory committees; BeiGene: Honoraria, Membership on an entity's Board of Directors or advisory committees.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal